Reception: +353 1 556 7900 | Mon – Fri: 8am – 4pm | Sat & Sun: 9am – 12pm by appointment only
- Treatments & Services
- All Fertility Tests
- Fertility Tests
- Ultrasound Scanning
- Tubal Patency Check
- Hormone Blood Tests
- Semen Analysis
- Other Tests
- First Step Package
Fertility Treatments- All Fertility Treatments
- Follicle Tracking
- Ovulation Induction
- Intra-uterine insemination
- In Vitro Fertilization
- Frozen Embryo Transfer
- Intracytoplasmic Sperm Injection
- Surrogacy
Male Factor- All Male Factor Services
- Semen Analysis
- Sperm Freezing
- Advanced Techniques
- Surgical Sperm Retrieval
- microTESE
Donor ServicesFertility Preservation- All Fertility Preservation Services
- Egg Freezing
- Sperm Freezing
- Embryo Freezing
- Before or After Cancer
- Childhood and Adolescent Cancer Fertility Project
- Late Adolescent Fertility Preservation
- Transgender Services
Fertility Treatments
Offering evidence-based, leading-edge treatments that provide potential pathways for you to create your family.
Follicle Tracking
When a woman is ovulating normally, an egg is released from the ovary during each menstrual cycle.
Eggs develop inside fluid-filled sacs, called follicles. Just prior to ovulation, follicles reach a size of around 20mm and can be seen on an ultrasound scan.
How is follicle tracking carried out?
Transvaginal ultrasound scanning can be used to monitor follicle growth and predict ovulation.
When is follicle tracking used?
Follicle tracking allows us to monitor follicle development so that intercourse can be timed around ovulation. Follicle tracking and TSI (timed sexual intercourse) is only used when:
- ovaries are producing follicles
- semen analysis are in a normal range
- fallopian tubes and pelvis are also normal
Follicle tracking may be useful for women whose cycles are very irregular and unpredictable.
Ovulation Induction (OI)
Ovulation induction (OI) refers to the use of fertility medication to cause ovulation in a woman who might not ovulate spontaneously.
Fertility medications used include tablets such as Clomid, Tamoxifen or Letrozole, or injections of the hormones Follicle Stimulating Hormone (FSH) or Luteinizing Hormone (LH). These may also be used in women who do ovulate in order to ‘boost’ ovulation, a process that is referred to as superovulation.
Monitoring ovulation
The dose of fertility drug used is critical and varies from woman to woman. Some women may over-respond to a particular dose while others may not respond at all. Close monitoring of developing follicles, which contain the eggs, is carried out using using transvaginal ultrasound scanning.
Once the follicles reach the correct size (around 20mm), ovulation is likely to occur within 48 hours. The couple are advised to have intercourse over the following days.

Intra-uterine insemination (IUI)
This treatment aims to place sperm in the uterus at the time when there is an egg available to fertilise. When performing an IUI treatment, healthy sperm are separated from a semen sample and placed into the uterus using a very soft, thin tube in a procedure like a smear test.
How is IUI timed?
IUI must be performed around the time of ovulation. The woman’s cycle is monitored using vaginal ultrasound scanning to ensure the sperm are added when the egg is ready. IUI may be performed during a natural, unmedicated cycle or in combination with fertility medication.
When is IUI recommended?
IUI is recommended as a fertility treatment for mild sperm abnormalities, cervical problems or where psycho-sexual issues may exist. It is normally recommended for women less than 37 years, thought there may be exceptions depending on individual circumstances. It may also be a good option for same sex female couples.
IUI is not recommended if there is significant endometriosis (grades III – IV), tubal disease (e.g. following tubal infection), significant sperm abnormalities or in older women.

In Vitro Fertilization (IVF)
IVF
In vitro fertilization literally means ‘fertilized in glass’. In IVF, eggs are removed from the ovary just before ovulation. The eggs are then placed, together with sperm, in a specialised laboratory environment.
Sperm compete to fertilise the egg, and the next morning, the embryology team check each egg. Those that have successfully fertilised are then allowed to develop for between three to six days in the laboratory
When is IVF used?
IVF was originally developed to treat blocked and damaged fallopian tubes. Now, IVF is used for a wide range of fertility issues including endometriosis and unexplained infertility.
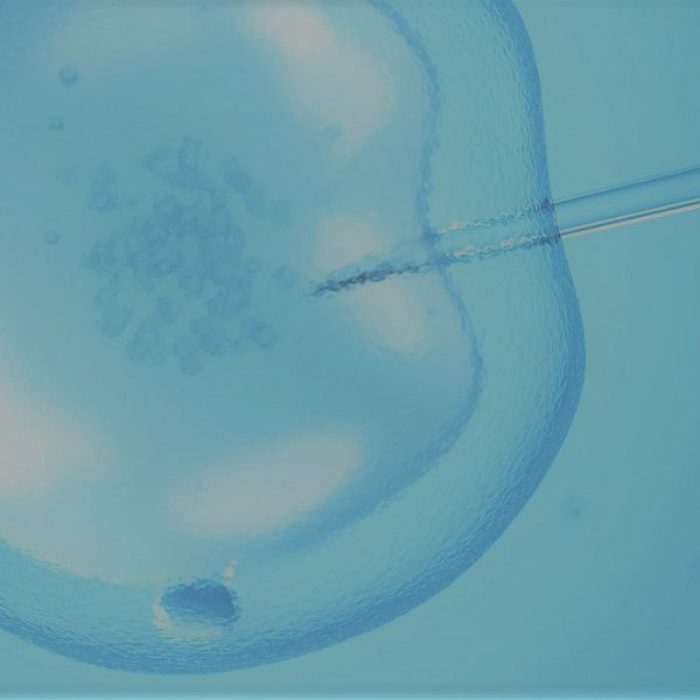
Intracytoplasmic Sperm Injection (ICSI)
ICSI is a specialised form of IVF. In contrast to conventional IVF, where the sperm penetrates the egg itself, ICSI involves injecting a single sperm directly into an egg using a fine glass needle. All other stages of the treatment cycle are identical to IVF.
ICSI is recommended in cases where there are not enough motile sperm to fertilize an egg using IVF. It is particularly useful in cases where sperm parameters are severely reduced. ICSI is also used to fertilise eggs that have been frozen.
Steps in a cycle of IVF or ICSI
- 2 to 5 clinic monitoring visits, which are a combination of ultrasound scanning and blood tests
- 8 to 12 days of stimulation medication
- Trigger injection 36 hours before the egg retrieval
- Egg retrieval is carried out with sedation given by a Consultant Anaesthetist.
- Fertilisation of the egg and sperm to create embryos
- Transfer of a suitable embryo to the uterus, 3 to 5 days after the egg collection
EmbryoGlue®
This is a fluid or media that an embryo can be placed in before being transferred. It can support the process of the embryo implanting into the lining of the uterus, the next developmental step after transfer.
Embryo Freezing
Following embryo transfer, there may be other embryos of good quality.
These embryos can then be frozen or ‘cryopreserved’, stored. They can then be thawed for use later during a Frozen Embryo Transfer (FET) treatment cycle.
Not all embryos are suitable for freezing, they must be at least good quality.
Single Embryo Transfer Policy
Merrion Fertility Clinic has an elective single embryo transfer policy. For good prognosis patients, a single good quality embryo is transferred and any other good quality embryos are frozen for subsequent use.
Double embryo transfer may be recommended in certain situations. This option will be discussed with you before your embryo transfer.
Frozen Embryo Transfer
Some patients will have embryos frozen during their IVF/ICSI treatment cycle, for future use. A FET cycle involves thawing frozen embryos and transferring them back to the womb.
FET cycles are much simpler than fresh cycles, as ovulation induction, egg collection and fertilisation are not required.
Over 98% of vitrified embryos will survive the freezing process and be suitable for transfer when thawed.

Surrogacy
Surrogacy supports family creation where the intending parent or parents cannot carry a pregnancy. An embryo is created using the intending parents’ sperm and egg and transferred to the uterus of the surrogate. The surrogate carries the pregnancy but has no genetic connection with the child
Common medical indications for surrogacy are situations where women are born without a uterus, or where their uterus become injured or needs to be removed, for example from cancer, surgery or haemorrhage in pregnancy.
Other women have serious medical conditions where pregnancy could prove fatal to them and their babies. There are also some specific but rare causes of infertility and recurrent miscarriage where surrogacy may be advised.
Surrogacy is extremely complex from a legal point of view. The Assisted Human Reproduction Act was signed into law in 2024 but has not yet commenced. Until then, the provision of surrogacy in Ireland is licenced by the Health Products Regulatory Authority, the HPRA.
Merrion Fertility Clinic is licensed to provide surrogacy in Ireland. However, this licence has extremely strict requirements. These include a medical indication for surrogacy and patients must have a family member or close friend who is willing to act as a surrogate.
There are strict requirements also for the surrogate. All of those involved must be resident in Ireland and all must be willing to receive legal advice and attend counselling.
For those seeking surrogacy, the National Infertility and Support Group (NISIG) have outlined some important advice in their document on International Surrogacy.

Book a Consultation
If you are considering your fertility, why not book an online consult with one of our team of doctors?
